Important Safety Information
WARNING: ARTERIAL AND VENOUS THROMBOEMBOLIC COMPLICATIONS
Patients being treated with Vitamin K antagonist therapy have underlying disease states that predispose them to thromboembolic events. Potential benefits of reversing VKA should be weighed against the risk of thromboembolic events, especially in patients with history of such events. Resumption of anticoagulation therapy should be carefully considered once the risk of thromboembolic events outweighs the risk of acute bleeding. Both fatal and nonfatal arterial and venous thromboembolic complications have been reported in clinical trials and postmarketing surveillance. Monitor patients receiving KCENTRA, and inform them of signs and symptoms of thromboembolic events. KCENTRA was not studied in subjects who had a thromboembolic event, myocardial infarction, disseminated intravascular coagulation, cerebral vascular accident, transient ischemic attack, unstable angina pectoris, or severe peripheral vascular disease within the prior 3 months. KCENTRA might not be suitable for patients with thromboembolic events in the prior 3 months.
KCENTRA is contraindicated in patients with known anaphylactic or severe systemic reactions to KCENTRA or any of its components (including heparin, Factors II, VII, IX, X, Proteins C and S, Antithrombin III and human albumin). KCENTRA is also contraindicated in patients with disseminated intravascular coagulation. Because KCENTRA contains heparin, it is contraindicated in patients with heparin-induced thrombocytopenia (HIT).
Hypersensitivity reactions to KCENTRA may occur. If patient experiences severe allergic or anaphylactic type reactions, discontinue administration and institute appropriate treatment.
In clinical trials, the most frequent (≥2.8%) adverse reactions observed in subjects receiving KCENTRA were headache, nausea/vomiting, hypotension, and anemia. The most serious adverse reactions were thromboembolic events, including stroke, pulmonary embolism and deep vein thrombosis.
KCENTRA is derived from human plasma. The risk of transmission of infectious agents, including viruses and, theoretically, the Creutzfeldt-Jakob disease (CJD) agent and its variant (vCJD), cannot be completely eliminated.
Indications
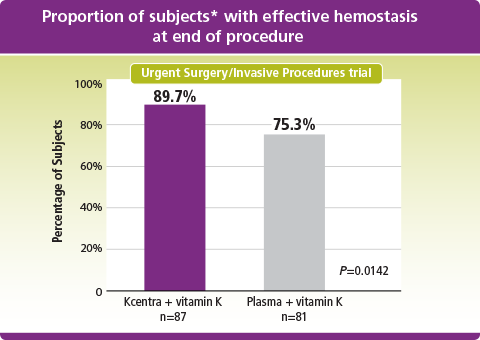
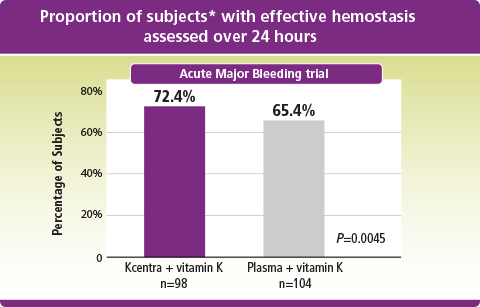
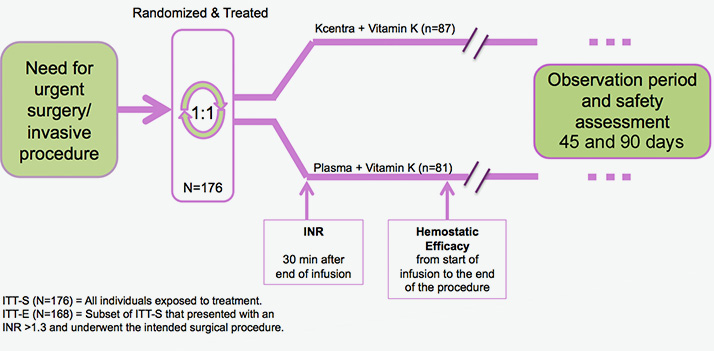
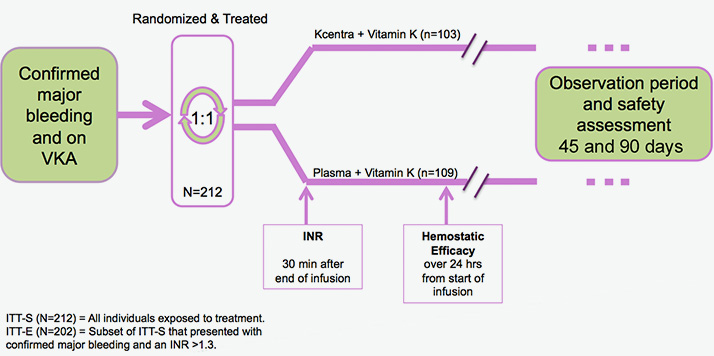
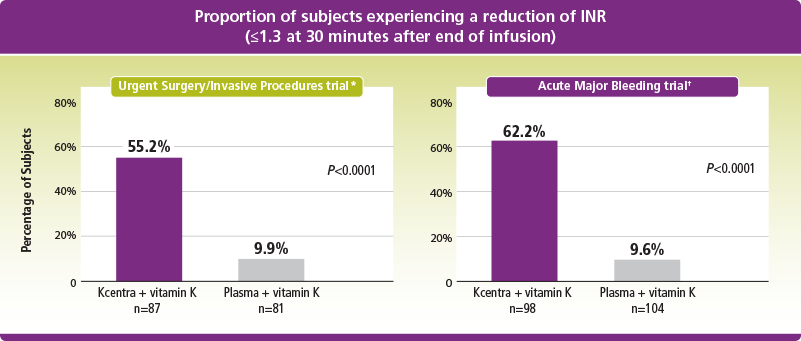
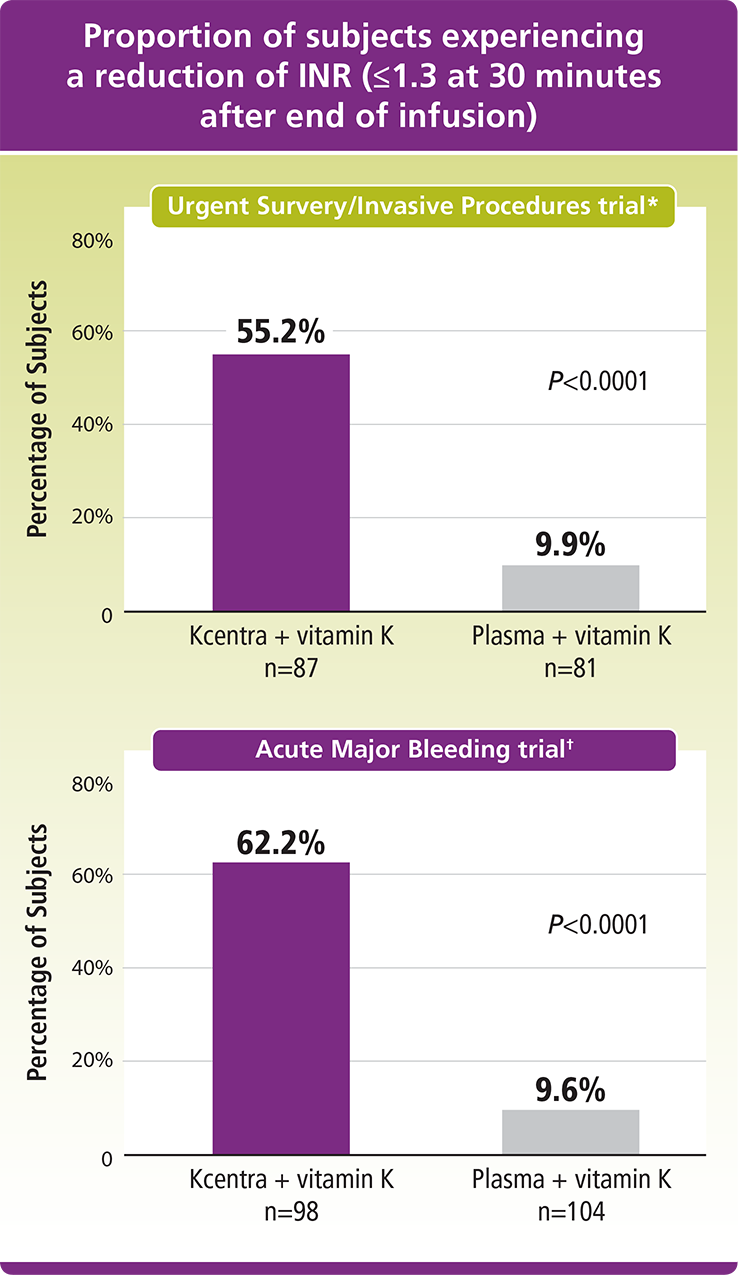
KCENTRA®, Prothrombin Complex Concentrate (Human), is a blood coagulation factor replacement product indicated for the urgent reversal of acquired coagulation factor deficiency induced by Vitamin K antagonist (VKA—eg, warfarin) therapy in adult patients with acute major bleeding or the need for urgent surgery or other invasive procedure. KCENTRA is for intravenous use only.
Please see full prescribing information for KCENTRA.
To report SUSPECTED ADVERSE REACTIONS, contact the CSL Behring Pharmacovigilance Department at 1-866-915-6958 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.